The other day I was reading an article by my sector colleague Dr Luis Barbero where he was reflecting on the orthodontist profession in a blog of Smart Aligner Services and gave me pause for thought.
In 2024, with almost a quarter of a new century behind us, orthodontics continues to undergo major technical changes that involve alternatives that would have been unthinkable a few years ago, mainly due to the incorporation of skeletal anchorage into our daily routine as a complement to treatment with fixed orthodontics or aligners, and even for the treatment of disjunctions in adults.
However, it is important to remember that although the potential of these tools is enormous, orthodontic diagnosis and the principles governing occlusion and the relationship between teeth and their bony bases remain the same as they were a century ago.
A decade ago Janson et al published a very interesting article (Janson G, Maria FR, Bombonatti R. Frequency evaluation of different extraction protocols in orthodontic treatment during 35 years. Prog Orthod. 2014;15(1):51.) in which they concluded that the frequency of the non-extraction protocol gradually increased from 14.29% (1973 to 1977, interval 1 in the table below) to 54.55% (2003 to 2007, interval 7 in the table below).
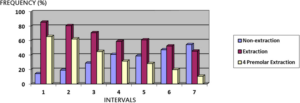
In addition, they found that the frequency of the four premolar extraction protocol gradually decreased from 65.72% (1973 to 1977) to10.72% (2003 to 2007), while the two maxillary premolar extraction protocol has shown the same frequency of indications over the same time period.
This last point is interesting: extractions fall in the lower jaw... although the growth potential of the lower jaw is limited with standard orthodontic clinic techniques that do not include an orthognathic approach.
Looking back, Ricketts (Ricketts RM. A principle of arcial growth of the mandible. Angle Orthod. 1972 Oct;42(4):368-86.) would have told us that mandibular third molars should be extracted if premolar extractions are not going to be performed as part of the planned treatment, as 45% of a group of patients treated without premolar extractions ended up needing third molar extractions.
Something that is also not done.
Moreover, in the same article, he points out that between 15% and 20% of orthodontic patients need third molar extractions, even when premolar extractions are part of active orthodontic treatment.
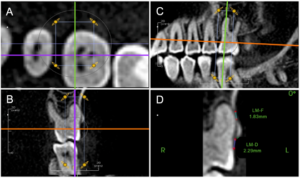
When asked the question, do we make fewer extractions than we should? The answer is yesThe more recent literature (Allahham DO, Kotsailidi EA, Barmak AB, Rossouw PE, El-Bialy T, Michelogiannakis D. Association between nonextraction clear aligner therapy and alveolar bone dehiscences and fenestrations in adults with mild-to-moderate crowding. Am J Orthod Dentofacial Orthop. 2023 Jan;163(1):22-32.e4) suggests a high number of fenestrations and dehiscences resulting from dental overexpansion beyond the limits of both jaws, even with moderate crowding.
Perhaps we should rethink whether we dedicate enough time to communicate the importance of extractions to our patients, and whether we are really aware of the importance of a careful diagnosis and a treatment plan that takes into account orthodontic and periodontal criteria... whatever technique we use.